













 11 / 24
11 / 24

SUMMER 2015 ISSUE
EQUINE MATTERS
10
GRASS SICKNESS
Clinical signs
Within the literature, extensive reference is
made to EGS presenting clinically as one
of three forms: acute, subacute and chronic.
These are classified according to the duration
of disease however there is an inevitable
overlap between these sub-classifications
because disease duration is dependent on
severity, interventional factors, supportive care
and elective euthanasia.
The following clinical signs can be seen in
all cases of EGS:
●
Dullness
●
Anorexia
●
Mild to moderate colic
●
Difficulty swallowing: (dysphagia)
(Figure 1)
●
High heart rate
●
Drooping eyelids (ptosis)
(Figure 2)
●
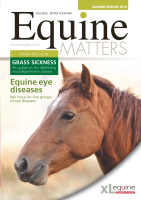
Patchy sweating
(Figure 3)
●
Muscle twitching
●
Dry, mucus covered faeces per rectum
Acute EGS (1-2 days):
●
Mild to moderate abdominal pain
●
Large volumes of nasogastric reflux
●
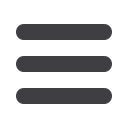
Small intestinal distension per rectum or
identified by an ultrasound scan
(Figure 4)
Subacute EGS (2-7 days):
●
Similar to acute cases but typically only
mild abdominal pain
●
Nasogastric reflux is not usually present
Chronic EGS (>7 days):
●
Weight loss leading to a greyhound,
tucked up appearance
●
Weight shifting of the hindlimbs, leaning
back against the walls
●
Inflammation and dryness of the nostrils
Diagnosis
A presumptive diagnosis is usually made
based on the nature and progression of
clinical signs, recent clinical history,
epidemological information and the ruling
out of other differential diagnoses.
Gold standard diagnosis is based on
examination of nerve bundles found within
an intestinal biopsy that is taken during an
exploratory colic surgery. Unfortunately, this
is often a post mortem examination as a
suitable ante mortem test is still unavailable.
One test to aid diagnosis is the reversal
of ptosis (drooping eyelids) following
administration of (0.05%) phenylephrine
eye drops. Unfortunately, the sensitivity
and specificity of these tests are not
significant enough to be used solely in
the diagnosis of EGS.
Figure 3: Patchy sweating seen across
the body
Figure 4: Distended small intestine can be
identified ultrasonographically
Treatment
Acute and subacute cases are associated
with a 95% mortality rate. However, fluid
therapy, analgesia and regular stomach
tubing can be initiated until a definitive
diagnosis can be achieved. At this stage,
euthanasia is recommended.
Chronic cases of EGS should be carefully
evaluated prior to euthanasia as up to 40%
can survive with appropriate nursing care.
The positive criteria to consider for chronic
cases includes:
●
Ability/willingness to drink and swallow
feed
●
Absence of continuous moderate to
serious colic signs
Treatment of chronic EGS:
The major concern for the chronic cases
of EGS to overcome is the profound
inappetance exhibited. A picnic of highly
palatable, good quality feeds that are high
in protein and energy should be provided.
Feeding preferences of these horses often
change regularly so different options should
be available for them.
In some cases, horses can be hospitalised
and administered nutrition by either continual
flow system or within the fluids intravenously.
There is not sufficient evidence to show
whether these regimes will improve the
outcome of the case but they will reduce
weight loss and consequently increase the
time available for spontaneous improvement
in appetite to be made.
Nursing care:
●
Pain relief as necessary
●
Regular hand feeding
●
Regular short walks/turnout periods at
grass
●
Antibiotics in cases where there is
evidence of feed inhalation to prevent
the development of inhalational
pneumonia
The nursing care of these cases requires
dedication, commitment and time from the
owner. It can take weeks to months for
improvements to be made and it is difficult
to predict whether the horse will survive
despite these efforts.
Research studies have shown that the
severity of swallowing difficulty, colic,
inappetance and rhinitis (inflammation of
nasal passages) is greater in non-survivors.
Cases which regain their appetite and their
body weight will often return to the same
level of strenuous exercise. However, even
in these cases, residual signs such as some
difficulty swallowing, intermittent colic and
coat changes can persist.
Prevention/vaccination
Last year, the Animal Health Trust, in
collaboration with the Universities of
Edinburgh, Liverpool and Surrey,
launched a randomised, placebo-
controlled field trial for a potential
vaccine. To qualify for inclusion with this
trial, horses must be kept at premises
that have been affected by at least one
EGS case within the preceding three
years. Horses are assigned to one of
two groups:
●
A vaccine group vaccinated with C
Botulinum Type C toxoid vaccine
●
A placebo group receiving inactive
placebo injection
The vaccine programme consists of three
injections at 21 day intervals, followed
by a booster vaccine at 12 months. The
horses remain under the care of their
normal veterinary practice and all visits,
vaccines, health checks are paid for by
the trial. The vaccine trial, if successful
will provide a major breakthrough in EGS
prevention. If you have suitable cases for
enrolment you are encouraged to contact
the EGS vaccine field team
at the Animal Health Trust
(equinegrasssickness@aht.org.ukor
telephone 01638 555399)
.