













 5 / 24
5 / 24

A full lameness examination should be
performed which may include lunging,
observation under saddle, flexion and
extension and frog pressure tests. A physical
examination including the use of hoof testers
will also be carried out. Your vet may at this
point be highly suspicious of foot pain. The
location of pain within the foot can be
evaluated with the use of nerve blocks and
blocks of the coffin joint and navicular bursa.
If pain in the foot is confirmed, a radiographic
examination will be performed next. After shoe
removal and foot preparation, numerous x-ray
views of the foot will be taken to check for the
presence, number, shape, size and location of
specific degenerative changes and an
assessment will be made of bone definition
and regularity, and new bone growth.
Bone scans (scintigraphy), CT or MRI scans
may also be performed. MRI will be most
commonly used to more accurately assess
the tendons, ligaments and give us vital
information about the bone that can’t be seen
on x-ray, such as bone necrosis, fibrosis or
haemorrhage. Bursoscopy is occasional done
to directly see the fibrocartilage at the back of
the navicular bone and the deep digital flexor
tendon and any adhesions between them.
Corrective farriery is the mainstay of
treatment with our first goal being to get the
foot back in perfect balance. As some cases
can have ‘long toe, low heel’ conformations
and others could have small upright boxy
feet, there is no single way to trim and
shoe navicular disease cases. Every horse
is an individual.
We can say however that we want to ensure
a straight hoof pastern axis and correct
side-to-side balance. We want plenty of
support for the caudal heel to expand and
contract, and nails shouldn’t be put too far
back. The break over point should be as far
back as possible to encourage early take
off and reduce the stress on the navicular
apparatus. Your vet and farrier may decide
together that egg bar shoes, natural balance
shoes or heart bar shoes are appropriate.
They may decide your horse needs
graduated shoes or wedges or possibly just
a wide web shoe with a little extra length.
Solar packing may be advised.
Additional medical treatments may be used.
This may include anti-inflammatory painkillers
such as phenylbutazone or steroids may be
injected directly into the navicular bursa. Your
vet may recommend bisphosphonate drugs,
such as clodronate, which helps to reduce
further weakening of the navicular bone.
Isoxuprine can be used as a vasodilator to
improve blood flow to the foot although this
treatment has gone somewhat out of fashion.
Short-term pain relief can be obtained by
using extracorporeal shock wave therapy
(ECSWT).
In advanced cases, chemical or surgical
intervention of the pain conducting nerves
may be warranted. Freezing the nerves
with liquid nitrogen or injecting alcohol,
sarapin or even cobra venom around the
nerves to the foot to alleviate pain, have
been reported. Surgical procedures can be
performed involving severing supporting
ligaments (desmotomy). Pain relief can also
be achieved by directly cutting the nerves
(neurectomy) to the heel/foot. This can
give up to 18 months relief before sensation
appears to come back.
NAV I CULAR D I SEASE
SUMMER 2015 ISSUE
EQUINE MATTERS
4
Note the front wall, heel and pastern are
all parallel
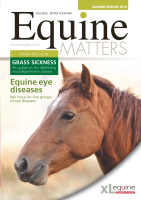
Radiography has historically been the
primary method of diagnosing cases of
navicular disease
Solar packing provides support and reduces
the stress on the navicular apparatus
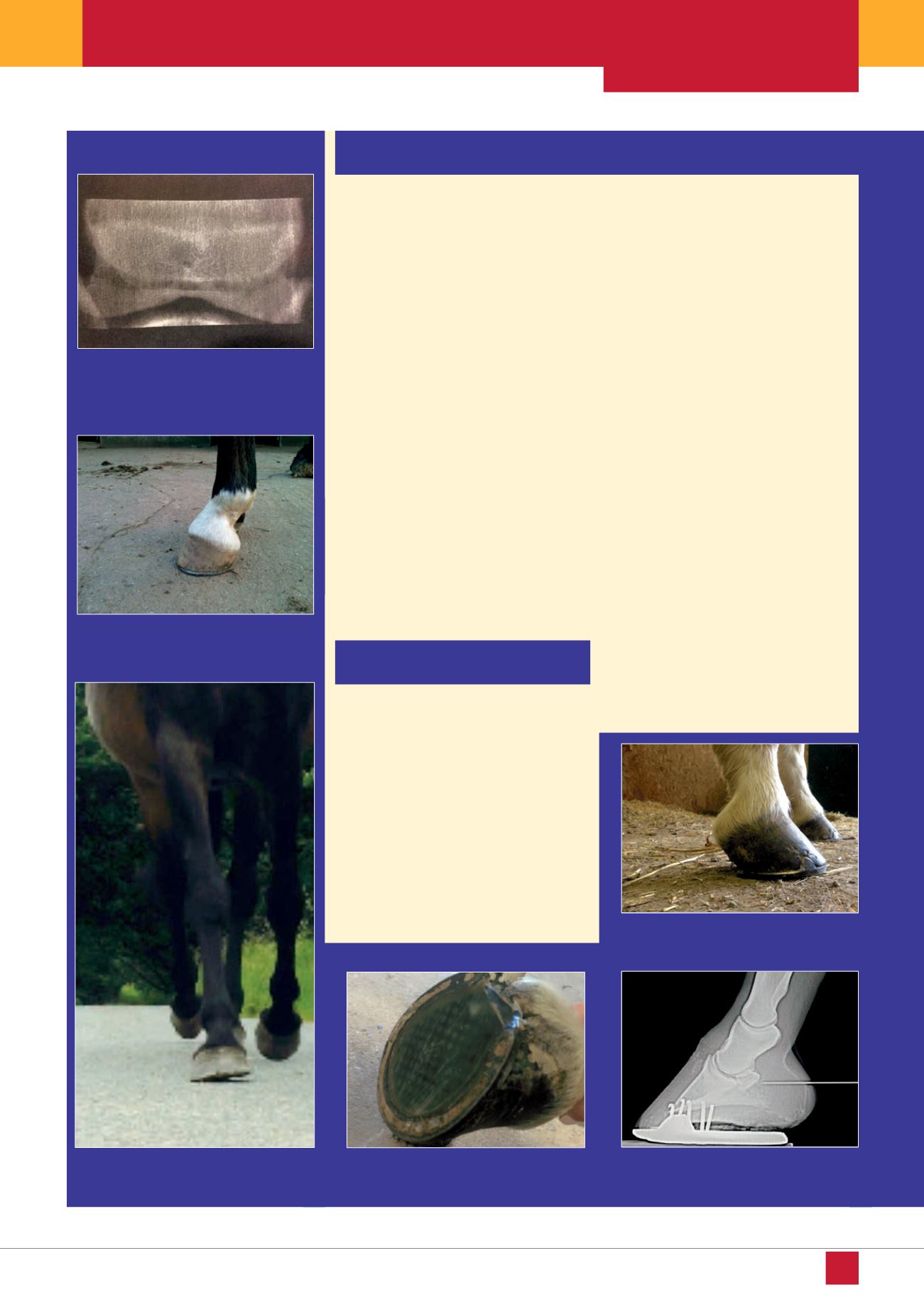
Dynamic and static foot balance should be
assessed and treated
X-ray guided medication of the navicular
bursa
Treatment options for navicular
disease
Diagnosis
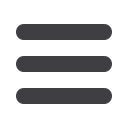
A broken-back hoof pastern axis can cause
low grade cumulative injury