














 7 / 24
7 / 24

SPRING 2016 ISSUE
EQUINE MATTERS
6
Nuclear scintigraphy
Nuclear scintigraphy or bone scanning is most
commonly used in the investigation of under
performing horses where the cause of the
problem is not clear and a general approach
is required, or when multiple limbs are
affected. Often horses are not obviously lame,
rather just lacking propulsion or disuniting at
canter. A radioactive phosphate molecule is
injected into the horse’s bloodstream which
binds to the bones of the skeleton. Any areas
of the skeleton which are damaged will bind
more of the molecule than normal and will be
visible when images are taken with a gamma
camera. The entire skeleton can be examined
in a single session (taking about two hours)
with the horse under standing sedation. Bone
scanning is particularly important for diagnosis
of back and pelvis injuries
(figures 1 and 2)
,
but is also useful for head, neck and leg
issues. Once the problem area is identified,
further imaging such as radiography will likely
be required to characterise the exact nature of
the injury.
Magnetic resonance imaging
MRI gives an extremely detailed three
dimensional view of all types of tissues, but
can only examine small areas at a time. Most
machines are currently only large enough to
allow imaging from the top of the cannon
downwards, and examination is limited to
a single area at a time, e.g. the fetlock
(figure 3)
. The area to be examined is placed
inside a powerful magnet and radio waves
are applied. The signal produced varies
according to different tissue characteristics,
allowing a computer to create an image of
the horse’s leg in which all the different tissues
can be clearly identified and analysed for any
abnormalities. MRI is indicated when the
location of a cause of lameness has to be
regionalised, usually with nerve blocks, but
conventional imaging modalities have not
identified the problem. It is most commonly
used to examine horses’ front feet
(figure 4)
and has significantly improved our
understanding and management of foot pain.
Computed Tomography
CT is essentially a three dimensional
radiograph. The area to be examined is
placed inside a helical x-ray generator and
images are taken in a circular fashion.
Using a computer, a 3D image can then
be developed which provides detailed
information of the position and density
of adjacent tissues and avoids the
superimposition of tissues which plagues
standard 2D radiographs. CT is most
commonly performed in standing horses
to examine the head for dental or sinus
disease, or the neck for causes of
incoordination (Wobbler's Syndrome).
CT is also used in anaesthetised patients to
examine the legs, allowing appreciation of
complex fractures prior to reconstructive
surgery, or in combination with a contrast
agent to look at soft tissue disease. In some
cases it is now possible to get a horse’s
stifle into a CT machine to investigate the
joint cartilages and cruciate ligaments.
As in human medicine, diagnostic imaging
for equine patients is advancing rapidly.
Machines are becoming larger and more
powerful every year, allowing more areas
of the horse to be examined and more
detailed images to be produced. Perhaps
the days of a ‘whole horse scan’ are not
that far away.
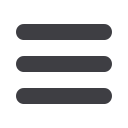
Figure 1. Bone scan of the back. Nuclear scintigraphy image of the
left side of a horse’s back. A clear ‘hot spot’ is seen at the centre of
the back, directly under the weight of the rider. This is indicative of
‘kissing spines’ (blue arrow).
ADVANCED IMAGING
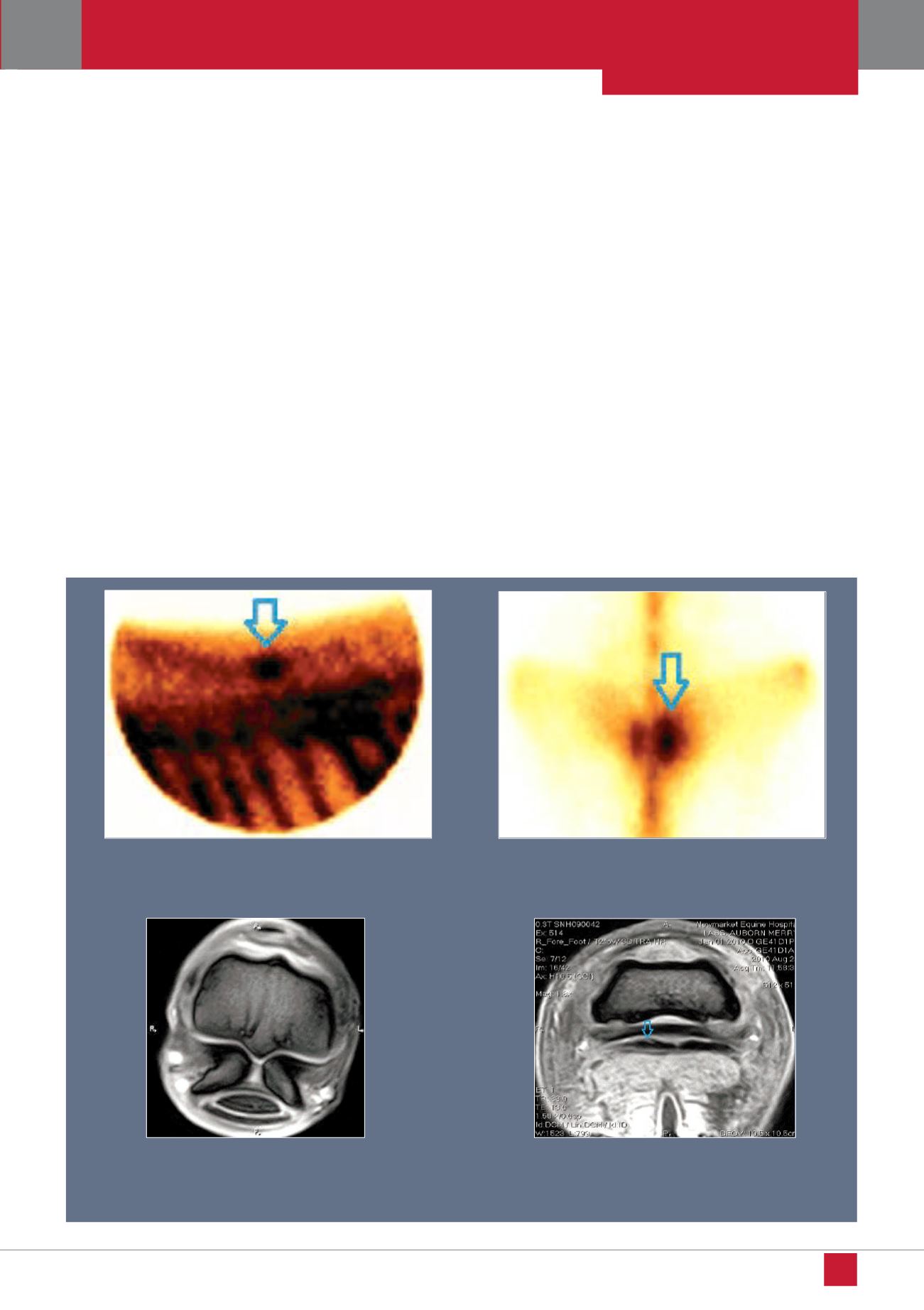
Figure 3. MRI fetlock.
MRI image of a normal horse’s fetlock joint
taken parallel to ground level. Excellent detail of bone density,
cartilage thickness and tendon integrity can all be seen on the same
image.
Figure 2. Bone scan of the pelvis.
Nuclear scintigraphy image of
a horse’s pelvis from above. There is much more uptake of the
radioactive ‘dye’ in the right sacroiliac region when compared
with the left (blue arrow), indicating right sided sacroiliac disease.
Figure 4. MRI Foot.
MRI image of a horse’s foot taken parallel to
ground level. A tear can be seen in the deep digital flexor tendon
(see blue arrow above). This injury is not visible on radiographs
and due to the structure of the hoof, cannot be easily identified by
ultrasound examination.